Sage Advocacy
Introduction
Sage Advocacy is the National Advocacy Service for Older People. It also supports vulnerable adults,
including survivors of institutional abuse and it supports healthcare patients in certain situations
where no other service is available to assist. This submission on the Covid-19 evaluation is based on
the experience and perspectives of Sage personnel working as independent advocates and trying to
deliver the best possible service in a challenging environment.
Sage Advocacy, because of the involvement of its frontline staff with vulnerable adults throughout
Covid-19, is well placed to have a good insight into what happened and why. Also relevant is the fact
that Sage advocates are independent of the health and social care system and, therefore, in a
position to make objective observations.
The submission is set out under the following headings:
– Nursing home care: the challenges presented by Covid-191
– Home care supports
– Hospital discharges
-The impact of the media and reporting on how people experience the pandemic
– Mental health issues associated with the pandemic
– Overview of Sage Advocacy perspectives
– How Ireland responded to the Covid-19 crisis: Observations by Sage Advocacy
– Critical overarching matters
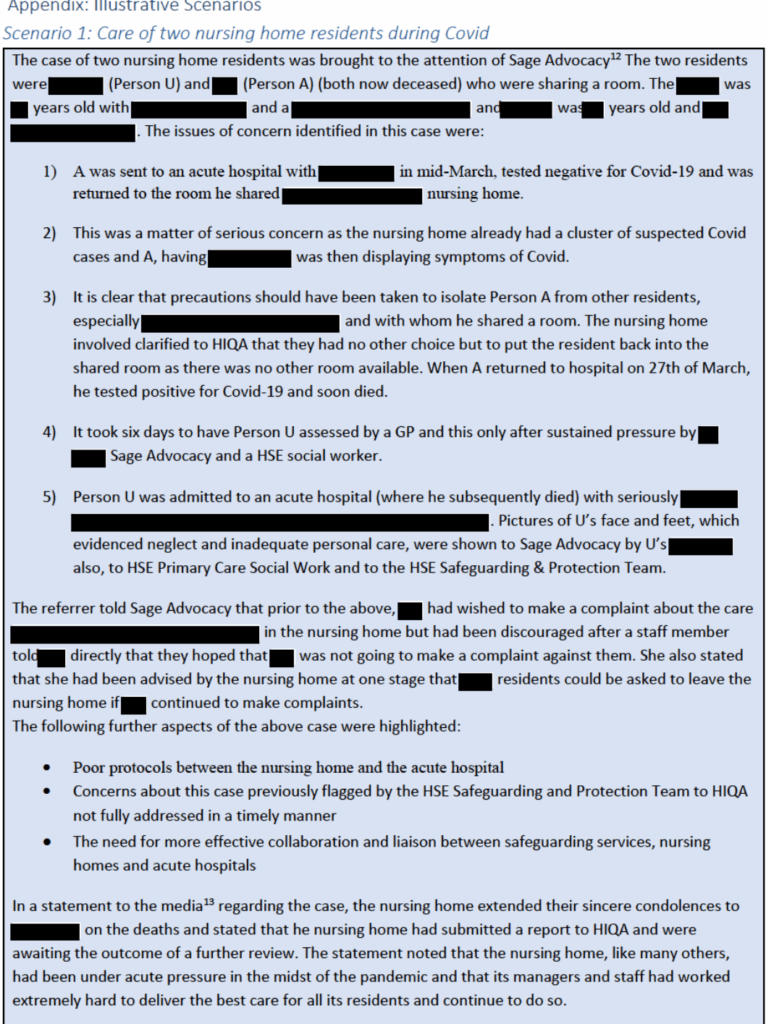
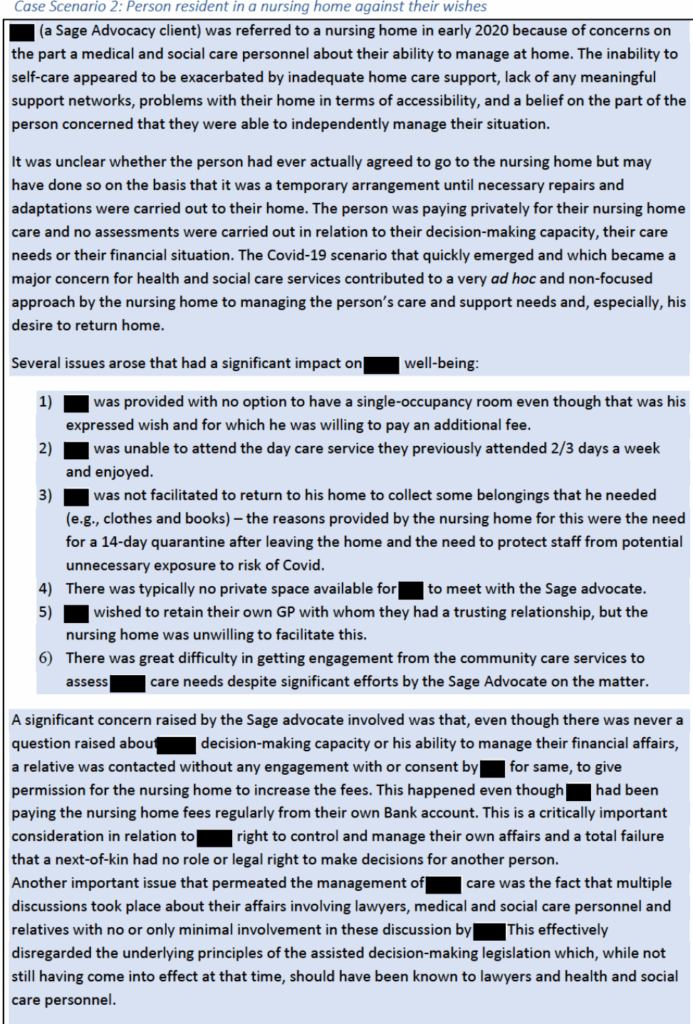
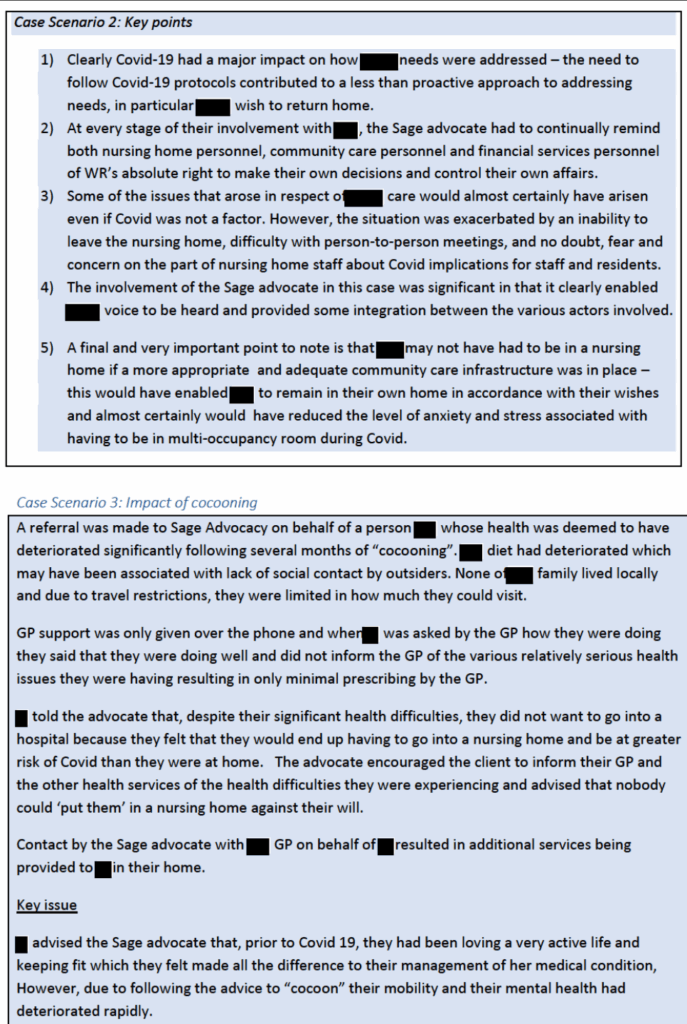
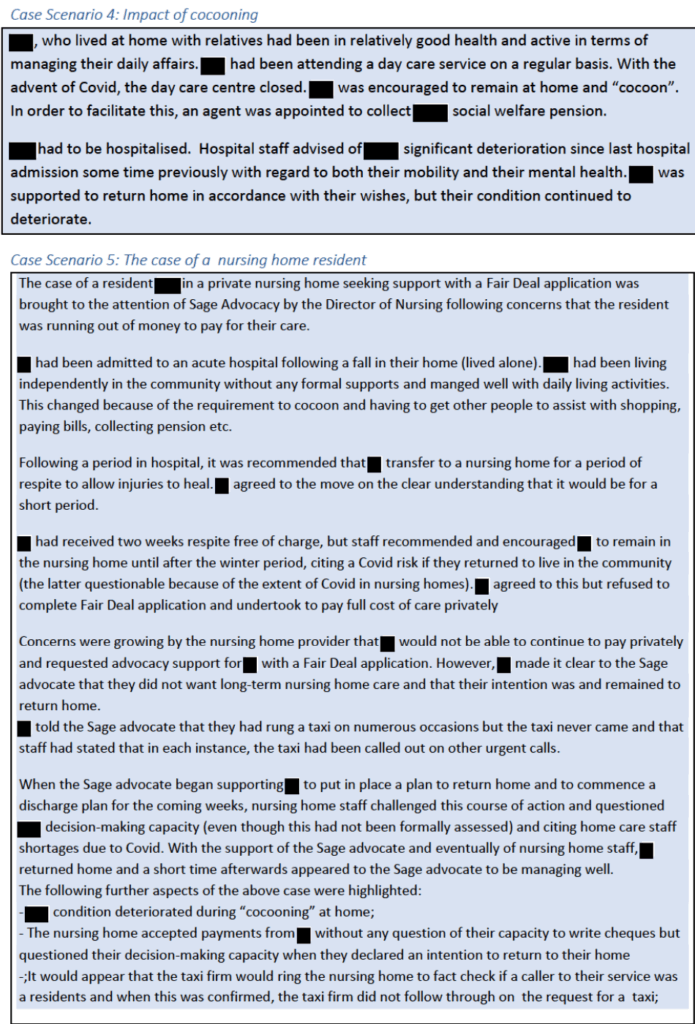
An Appendix included contains a series of vignettes which illustrate the issues referenced in the
submission. These are based on Sage Advocacy casework.
A critical underlying factor in the way Covid-19 impacted on at-risk older persons (many of whom
were already Sage clients or who would have required independent advocacy support) was the then
(and indeed ongoing) very high reliance on residential nursing homes to provide care and support.
This is an important issue going forward which needs to be addressed by: (i) reducing the number of
people in nursing homes on a long-term basis; and (ii) ensuring that provision is made for access by
residents to independent advocacy during times of crisis.
Nursing home care: The challenges presented by Covid-19
The issues identified by Sage Advocacy relating to nursing homes broadly mirrors the findings of the
various review groups – the Oireachtas Special Committee on Covid-19 Response2
, the Covid-19 Nursing Homes Expert Panel3, HIQA4.
.These include inadequate clinical oversight in private nursing
homes, a total lack of any protocols at the outset of the pandemic between the HSE and the private
nursing home sector and the continued use of multi-occupancy rooms and outmoded premises in
some nursing homes.
The major focus by Government, the HSE and the Department of Health at the outset of the
pandemic was on preparing hospitals and Intensive Care Units for an influx of Covid-19 related
admissions, with nursing homes (especially private nursing homes) and the residential care sector
generally being largely forgotten. In an effort to clear much needed acute hospital beds, discharges
to nursing homes were accelerated, with a high number of patients receiving transitional care
funding for a long period. Sage Advocacy received feedback from nursing homes confirming that
sometimes residents arrived in the nursing homes very late at night or during the weekend, without
any prior assessment or adequate notice.
Casework during the pandemic showed that in certain situations, when the residents received
transitional care funding indefinitely, there was no proactive engagement with professionals to
clarify the status of those placements – as a result, many residents were not actively supported to
return home or have the NHSS application completed.
Sage advocates received an influx of requests for support when the HSE began putting the nursing
home on notice regarding the termination of the transitional care funding for residents who were for
in receipt of it for a relatively long period.
Nursing home staffing and resource issues
There were huge staffing issues for private nursing homes both at the beginning of the pandemic
and throughout, with inadequate support being available from the HSE. While some of these issues
were eventually addressed by the HSE, staff shortages in private nursing homes and a heavy reliance
on agency staff continued to be an issue throughout the pandemic.
As testing for Covid became the norm for both residents and staff in nursing homes, this resulted in
many staff needing to self-isolate at home and nursing homes having to recruit agency staff. This
was seen as compounding an already difficult situation as some of these agency staff worked in
several different places of care in any given week. In addition, the use of agency staff inevitably
created additional stress and was disruptive for residents because of not personally knowing who
was going to be caring for them on any given day or night. In practice and in order to meet HIQA
requirements and to manage continuity of care, there were no alternative options available to
nursing homes.
Private nursing homes also highlighted to Sage Advocacy difficulties in attracting temporary staff,
citing the fact that the HSE pay was higher than the nursing homes could afford. While the Covid-19
social welfare payment was a very positive and necessary move to support people who became
unemployed, there was a question as to what extent the payment contributed to low paid staff in
the nursing home sector, e.g., care assistants and cleaning and catering staff, deciding to stay off
work and apply for the payment.
Having to rely on staff from “outside” the nursing home was problematic for nursing homes. In this
regard, it is noted that the Covid-19 Nursing Homes Expert Panel recommended that nursing homes
should have a clear written back-up plan when regular staff cannot work or fail to turn up for work
and that this should be incorporated into the nursing home’s preparedness plan for review by HIQA
(Recommendation 5.2). The Expert Panel also recommended that for the next 18 months (or until
the declaration of the end of the Global pandemic by the WHO), staff employed by a nursing home
should be precluded from working across multiple sites and adequate single-site employment
contracts should be put in place to support this (Recommendation 5.6).
Sage Advocacy strongly believes that this recommendation should be implemented on an ongoing
basis as far as possible.
Nursing home staff were perceived by Sage Advocacy as feeling isolated and alone and without clear
direction. They also became overwhelmed with additional paperwork (e.g., NHI guidance
information, HIQA reporting, applications for grants for PPE). Sage advocates had a sense of nursing
home staff becoming exhausted because of the additional workload due to staff shortages and
having to work extraordinarily long hours which became dysfunctional and unsustainable.
There was also the fact that staff were becoming increasingly anxious and worried about
themselves, the people in their care and their families and were on high alert coming to work every
day. Some DONs reported to Sage advocates of being very fearful at times as they struggled to
protect residents and staff and to reassure relatives.
Impact of visitor restrictions
The need for visitor restrictions in nursing homes was clear and many private nursing homes put in
place visiting restrictions from early March 2020. This had been recommended by Nursing Homes
Ireland (NHI) on 6th March and was subsequently adopted as HSE and Government policy about a
week later. While in many instances, nursing home residents were facilitated to remain in contact
with relatives via video chats and proactive weekly updates from the nursing home, such
arrangements failed to meet the needs of many residents and presented major difficulties for some,
particularly those with reduced decision-making capacity, and for their relatives.
Sage advocates noted at the time that Skype, Face Time and communicating through windows were
simply inappropriate for many nursing home residents and, for some people, likely to add to their
confusion, anxiety and distress. (Some two-thirds of nursing home residents are deemed to have
some degree of dementia).5
Sage was aware of situations where nursing homes were further restricting visitation because of staffing issues. In some sites, the activities coordinators were
“gatekeepers” of who came to visit and when. Advocates were contacted by relatives or friends of
residents when they experienced issues with communication or visitation access.
Some nursing homes adapted to the emerging situation and built in temporary spaces for visits and
had in place a booking system for that. At times, visitors found this problematic, when no visiting
time slots were available that would suit them, due to work or other care commitments.
Communication and information
There was a poor level of communication with relatives by some nursing homes regarding the status
of the virus in the nursing home. As the number of positive Covid-19 clusters in nursing homes rose,
some nursing homes were perceived by Sage advocates to have become more reticent about
providing information and were not answering phones which put further stress on relatives seeking
information on the level of Covid in the nursing home. The point was also made that pressures on
staff almost certainly resulted in phones being unanswered in some nursing homes.
Nursing homes with websites (which many did not have) were reported as having varying levels of
Covid-19 information available with links to the HSE website. Some nursing homes set up a group
text messaging service for families of residents and advocates with ongoing cases in these nursing
homes which provided updates on developments. Other nursing homes had pre-recorded voice
messages with updates on Covid-19. At the time Sage Advocacy put a Family Forum mechanism in
place in order to bridge the communication gap between nursing homes and relatives. This Forum
also helped to capture issues emerging from engagement between family members and nursing
homes.
HIQA Checklist for preparedness of nursing homes
It was the experience of Sage Advocacy that the HIQA self-assessment6 and protocol guidelines for
residential settings initiative was perceived negatively by some nursing homes in that they saw
HIQA’s regulatory and inspection role as not lending itself to providing a required supportive role.
While some nursing homes found the HIQA Checklist useful, the view, as reported to Sage
advocates, was that it came much too late. It was regarded by many nursing homes as reactive
rather than proactive since it was April 18th before HIQA was designated as the body responsible for
assessing nursing homes’ readiness to deal with the pandemic and April 21st before the Checklist was
issued. This was six weeks after the decision to restrict visitors to nursing homes was introduced.
Sage advocates also reported that some nursing homes considered the Checklist to be another
paper-based requirement in an already stressed workplace.
While it was acknowledged that HIQA plays an important role in monitoring standards in nursing
homes, some nursing homes told Sage advocates at the time that without immediate resources to
put in place HIQA recommendations, its usefulness in the Covid-19 crisis was somewhat limited. On
the positive side, Sage advocates noted that in instances where they brought issues to HIQA’s
attention, HIQA staff encouraged families of nursing home residents to contact them with any
questions or concerns.
Involvement by Sage advocates in nursing homes
The support of an independent advocate was regarded by Sage Advocacy as critical for nursing home
residents during Covid and Sage Advocacy continued to try and provide an advocacy service in
nursing homes. However, this offer received somewhat of a mixed reaction with some nursing
homes simply not engaging with Sage, others referring residents who could be helped by means of a
telephone conversation and many using the link with Sage Advocates to articulate their multifaceted concerns and fears for their residents and staff and the pressures they were under on a daily
basis. Many of these pressures arose because of lack of HSE support initially, difficulty in getting
adequate PPE initially and subsequently an inability to roster a sufficient number of staff.
Sage Advocacy is in no doubt that, because of the lack of face-to- face independent advocacy
support over a prolonged period, many nursing home residents (some of whom were already Sage
clients) were put at greater risk in that their ‘voice’ simply was not heard for a prolonged period. In
some instances, referral to Sage Advocacy only happened when nursing homes’ income from
transitional care funding became problematic.
Also, in situations with complex family dynamics, the advocates were the ones liaising with different
“sections” of the family, keeping them informed, as the nursing home would have only issued a
message to one family contact.
Good practice in nursing homes
While there were many issues and difficulties that arose in nursing homes because of the pandemic,
there were also good stories which need to be told. Clearly, there is learning for future practice here.
Indeed, some nursing homes told Sage advocates that they were receiving good support from the
HSE and local GPs in the care of residents. Some Sage advocates reported having conversations with
residents in nursing homes who were very happy with the care that they received during the crisis.
There were a number of examples of good practice in nursing homes reported to Sage Advocacy:
– A rapid access team was set up in one nursing home to react to Covid-19 confirmed cases in
the home;
– Three separate dining rooms (for its 20 residents) were set up in one nursing home to
facilitate social distancing;
– Existing rooms were converted to ensure that each resident had their own room by making
use of, for example, an office, a chapel and a hairdresser’s room as additional bedrooms;
– Another nursing home instigated a Covid-19 testing system for a staff panel that they might
need to draw on as the pandemic evolved;
– Good practice was reported in an instance where in the case of death of a resident from a
non-Covid complication, a room was set up downstairs where the family could have access
without needing to enter the rest of nursing home;
– Regular Webinars were held in one CHO area connecting professionals from hospitals with
those in nursing homes or those working in the community;
Private nursing homes in the overall long-term care system
Sage advocates through their work and through media reports became aware early on in the
pandemic of the tension between private nursing homes and the HSE, particularly regarding the role
of the HSE as a provider of PPE to private nursing homes and in addressing the clear shortages of
staff in these homes. The nursing homes were represented as ‘for profit’ bodies who should look
after their own PPE while Nursing Homes Ireland (NHI) believed that the HSE was negligent in not
providing PPE to private nursing homes. It should be noted that the issue of PPE availability was
largely impacted on by the fact that the market was emptied of supply and that the HSE as a bulk
buyer could command priority purchasing.
The initial unilateral decision taken by NHI to restrict visitors was seen by Sage advocates as giving
the impression that private nursing homes had a plan and were in control of the situation. This
clearly turned out not to be the case. While nursing homes were not able to manage on their own,
on the other hand, as it emerged, the Department of Health and HSE did/do not have sufficient
linkages with the sector. This was regarded as a critical factor.
There was a lack of clarity as to who held the public health responsibility for nursing homes. Not
having a direct link with nursing homes, the HSE and the Department of Health relied on HIQA
which, while having an important regulatory and inspection role in respect of nursing homes, may
not have the in-depth insight as to what the shortfalls would be in the event of a pandemic such as
Covid-19.
While the pandemic was clearly a sharp learning curve for all involved, it is reasonable to suggest
that Directors of Public Health Nursing who manage community services within a defined
geographical area would have been much better placed to provide practical and clinical support to
the nursing homes in their patch and, thereby, discharge the public health responsibility more
effectively than was the case.
Other issues relating to nursing homes identified by Sage Advocacy at the time were:
– The delay in introducing Covid-19 testing in nursing homes was a critical factor.
– There was competition for available PPE at the outset and lack of clarity as to where
responsibility lay for providing the equipment to private nursing homes – this issue was
eventually resolved when ad hoc collaboration between public health services and private
nursing homes became the norm as the pandemic progressed.
– There was a perception on the part of Sage advocates at the time that, at least initially, the
promises of support staff from HSE were not adequately delivered. There was a sense that
the HSE provided oversight from its medical advisors but did not put in care assistants or
replacements for the latter when they became ill or took time off work to reduce the risk of
infection for themselves and their families.
– According to Nursing Homes Ireland, private nursing homes did not get the support that
they had been looking for and, if they had, they would not be in the position they were in.7
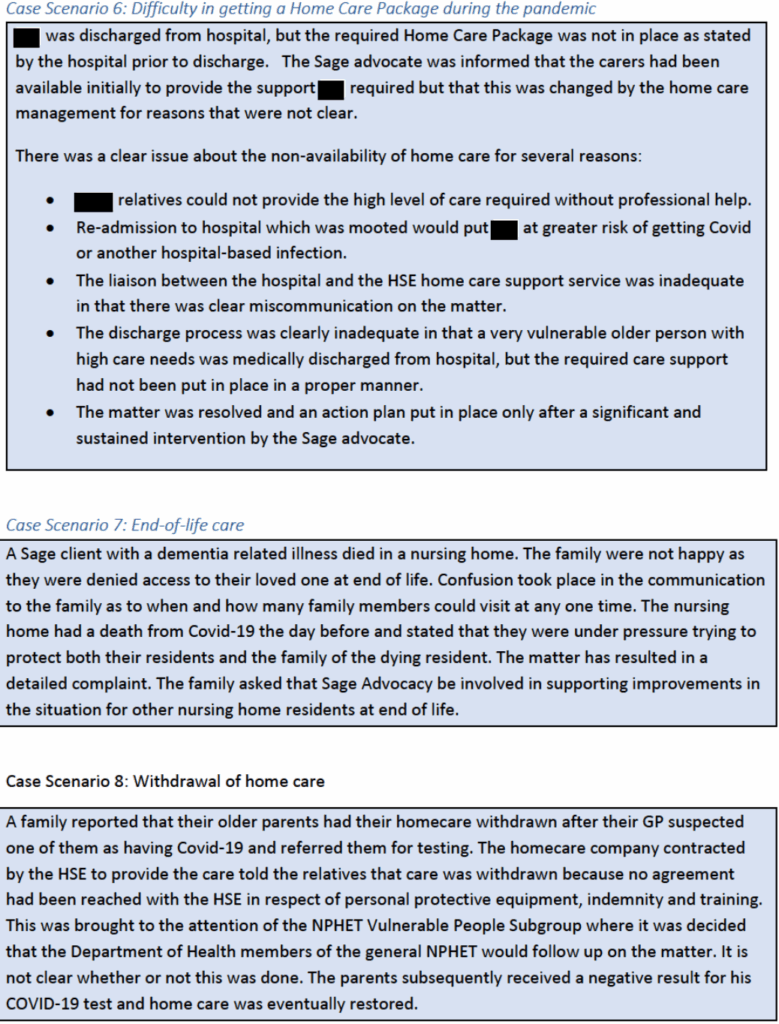
Home care supports
The provision of home care supports during the pandemic varied. On the one hand, there were
instances of people being discharged from acute hospitals with Home Care Packages (HCP) that were
adequate (and better than what would have been available prior to the onset of the pandemic)
while, on the other hand, there were instances where home care was either significantly reduced or
withdrawn.
Some home care providers indicated to Sage Advocacy that they lost a significant proportion of their
carers (25% in one case) due to people opting out of work because of the Covid-19 Payment (€350 a
week) or child-care issues or both. There were also instances of home care having to be refused to
new applicants due to carers being out sick or on leave due to fear of picking up Covid-19
themselves or infecting family members who had underlying conditions.
The overall impression of Sage advocates was that home support services remained in place for
people who had medium to high needs, including those who had suspected or confirmed Covid-19.
However, in some other situations, people with low support needs had some services reduced or
withdrawn. This was usually done after consultation with the person and their family. Alternative
supports were provided to many people in that situation through various voluntary supports. In
practice, as was widely acknowledged at the time, and highlighted in the media, in many areas,
community services came together and set up systems for checking in with older and vulnerable
people in the community who in some instances would not have been in receipt of any services.
However, Sage advocates became aware of instances where this did not happen and where there
were families who had not been linked into any community services prior to Covid-19 but who now
needed assistance.
Some home care providers indicated to Sage Advocacy that people had requested that the number
of calls to their home be reduced or the package suspended entirely due to Covid-19 concerns. In
some such cases, family members took on the role of providing the support required. However, it
was also brought to the attention of Sage Advocacy that this cancelling of the home care occurred in
some instances without any prior discussion with the person receiving the support and without their
consent. This was regarded by Sage advocates as a serious matter and an effective denial of a
person’s right to choose.
Some people working from home or who were off work and who were providing care to a relative
told Sage advocates that they were worried that the HCP would be taken away if they stated that
outside carers were not needed in the short-term. Therefore, some families were asking carers to
call but not to enter the home – this may have had the unintended consequence of further isolating
the person receiving the support.
While many positive initiatives were put in place, it is reasonable to suggest that supporting people
living at home could have been done much better. Engagement with families by home care
providers in exploring options, while satisfactory in some instances, was less so or non-existent in
other cases. Home care providers, regardless of whether HSE or private, should have been able to
assure families that they could meet all health and safety and PPE requirements. This did not always
happen and some families were left uncertain, frightened and forced into making decisions to carry
out care that in some cases was beyond their capacity and impacted negatively on the wellbeing and
mental and physical health of the whole household. While in many instances, families took over the
provision of care and support because of fear of outside carers bringing infection into the home, an
obvious concern was people unused to caring experiencing burn-out or tensions arising between
family members not usually spending so much time in a caring role. All this was happening while
children were being educated at home, parents were often working from home and physical
technology and broadband were far from ideal in many people’s homes.
The Covid-19 experience brought into sharp focus the inherent deficiencies in the community care
infrastructure. The reality was that many nursing home residents (at increased risk of exposure to
the virus) would not have been in that situation if there had been realistic care and support options
available to them in their own homes and in the community. The impact on the pandemic in nursing
homes should reinforce the point that more people should and could be cared for and supported in
either their own homes or in local-based small-scale sheltered/supported housing complexes, if the
latter were widely available.
Other points relating to home care identified by Sage advocates
✓ While there was some evidence of families taking their relative out of nursing home to
be cared for at home during Covid-19, there was also evidence of family members
blocking discharge home from a hospital due to Covid-19 concerns.
✓ There was some evidence of families refusing access to home carers because of fear that
the carers might be carrying the virus but be asymptomatic.
✓ Many home carers were not working because of fear of contacting the virus or because
they opted to avail of the social welfare Covid payment – this made it difficult to have a
consistent service.
✓ There was an additional difficulty for some people arising from having multiple carers,
many of whom were not previously known to them.
✓ The non-availability of respite/day services put enormous stress on families and further
isolated vulnerable older persons.
✓ The need to replace formal home care with phone contact presented a major difficulty
for people with reduced decision-making capacity who did not understand the need for
social distancing or why they could no longer meet carers that they liked.
✓ A number of PHN’s were redeployed during Covid which resulted in people living at
home being unable to access PHNs to help with care issues that arose for them.
Acute hospital discharges
A proactive discharge policy was taken by hospitals in response to the crisis. This resulted in
significant efforts being made to effect as many discharges of patients as possible in preparation for
an expected influx of Covid-19 patients.
Indeed, the typical ‘delayed discharge’ cases associated with waiting for a Home Care Package or
nursing home funding which was typical of the discharge process was no longer an issue. In this
regard, Sage Advocacy strongly believes that a key learning from the Covid experience should be
that this flexible discharge approach should become the norm with provision for easy access to home care packages.
However, this proactive approach to discharge was problematic because of the absence of a robust
Covid testing system. It is almost certain that that there would have been some transfers of Covid-19
positive patients back to the community as well as to nursing homes. Also, the asymptomatic nature
of Covid-19 in vulnerable older people was not understood in the early stages of the pandemic. This
point was highlighted by the Oireacthas Special Committee on Covid-19.8
It should also be noted also that there was also some commentary at the time about a higher than normal false negative in Covid-19 testing.9 The Covid-19 Nursing Homes Expert Panel recommended that all new nursing
home residents coming from the community or proposed transfers from hospitals should be tested
for Covid-19 prior to admission (Recommendation 4.1).
The impact of media reporting on how people experienced the pandemic
One line of media reporting which was facilitated by Government related to daily reporting on
numbers. This, perhaps unintentionally, communicated a message that may have had a ver
negative effect on people at risk of Covid. Typically, figures for the number of deaths that occurred
on any given day were accompanied by the statement that the median age of those who had died
was late 70s or 80s and/or that many had an underlying condition. This additional information, while
being a source of solace for much of the population who were fit and well and below that median
age, undoubtedly sent out a subliminal message about how we view our older people or those who
have an underlying condition.
Many nursing homes were experienced by Sage Advocacy as having been very concerned about their
nursing home being caught up in the media frenzy and being on ‘front pages of the papers’, where
the message might go out that they were non-compliant and failing to deal adequately with the
Covid-19 threat even though they had no cases in their nursing home or were managing the
challenge well.
The fact that many nursing homes were managing well with the resources at their disposal and
having no or only minimal case numbers was not adequately reported in the media. This resulted in
additional pressures on nursing homes, on residents and on residents’ relatives. While it was
acknowledged that the unpreparedness of nursing homes should be highlighted, there was also a
need for the media to publicise the fact that some nursing homes dealt with the challenge well.
Also, some nursing homes told Sage Advocacy that, while they floundered initially, they soon got on
top of the situation and that this was not reflected in media coverage.
Reluctance to attend hospitals
The focus in daily media reporting on Intensive Care Units and on the numbers of available hospital
beds and on numbers with Covid and related deaths almost certainly resulted in people with
conditions that needed medical intervention putting off going to a hospital. This may have had
significant consequences for older people who, as reported to Sage advocates, decided that there
was no point in going to a hospital and/or that it was unsafe to do so.
The initial media focus on inadequate PPE and the daily news reporting was seen by Sage advocates
as having created or amplified people’s fears about the dangers in going to their GP or to a hospital.
The media focus may have inadvertently communicated a message of GP surgeries and hospitals
being places to be avoided. This happened despite counter-messages coming from Government that
people should contact their GP and/or hospital if they had specific symptoms or conditions that
concerned them.
Media reports that large numbers of patients were discharged from acute hospitals to nursing
homes to prepare for the Covid-19 surge almost certainly resulted in adding to the already negative
image of nursing homes and a perception that they were being made warehouses for Covid-19
patients with all the associated risks, including death. There is a reasonable argument, based on the
number of Covid-related deaths in nursing homes, that this perception is accurate, notwithstanding
the fact that not all deaths categorised as Covid were actually because of Covid.
Also, media reports of nursing homes being short-staffed due to workers moving to the HSE for
better pay, while, perhaps, factually correct, put further stress on relatives of nursing home
residents.
Mental health issues arising from Covid-19: Perspectives of Sage advocates
People with mental health difficulties faced significant challenges during the pandemic. Their
situation was compounded by the fact that normal support and counselling services for those living
in the community had to be put in abeyance. In addition, vulnerable adults generally who were
‘locked down’ during Covid-19 were seen as almost certainly experiencing heightened anxiety
coupled with fear of infection. The increased burden of care on many families arising from the
suspension of home care provided by outsiders, the non-availability of day care centres and other
respite services was undoubtedly stressful for these families. Since people were not availing of GP
services as regularly as before Covid, it is almost certain that many vulnerable people were not
seeking or receiving the support that they needed to deal with this new situation.
The potential mental health impact on health care professionals working in a Covid-19 environment
is a matter that requires acknowledgement across the board. There was a clear need for additional
counselling supports going forward for people in residential care facilities, health care staff generally
as well as families in dealing with grief and coming to terms with what for many was a horrific
experience. There is little evidence that such supports were put in place at a level commensurate
with need.
Impact of isolation on nursing home residents
From an early stage in the pandemic, some relatives of people in nursing homes reported to Sage
Advocacy that they struggled to cope with not being able to visit their loved ones. This, coupled with
the fear of losing a loved one or a close relative being left to die alone added to their level of stress.
The isolation of residents in their rooms gave rise to serious concerns in relation to residents with
reduced decision-making capacity who did not understand the need to isolate and why they should
be confined to their rooms which was not their normal experience. Isolation was a particular
concern for many smaller nursing homes, especially older homes with few single rooms and where
residents had died from the virus.
Some nursing homes highlighted to Sage advocates the potential after-effects of restrictive practices
– keeping residents in their rooms during the lockdown and exclusion of visitors. The mental health
effects of being kept in one room for months were no doubt enormous (see below), particularly for
those with dementia. Some nursing home staff expressed worries to Sage advocates about the
human rights of residents in situations where they were being confined to their rooms.
While information booklets were distributed to every household that provided contact numbers for
mental health support services, there was little evidence that people knew that these services were
available or that they had any meaningful outreach into communities.
Mental health difficulties and possible post-traumatic stress disorder were regarded by Sage
Advocacy as becoming a huge issue in nursing homes following the pandemic – for residents, nursing
home staff and families.
Overview of Sage advocates’ experience during the pandemic
While Sage advocates had some difficulty in capturing the total picture in their catchment areas and
while there were notable divergences in practice between different CHO areas, the main picture that
emerged from feedback was that there were positive elements in the response of health and social
care services and, especially, by local communities.
The major focus on the role of the acute hospital in responding to the pandemic put pressure on
hospitals to discharge patients/older persons back home or to nursing homes. In contrast to the
situation prior to Covid-19, funding for such discharges was more easily accessible throughout the
pandemic.
The extent of the virus and related deaths in nursing homes was seen as a major shortcoming in our
long-term care and support system. Issues at the beginning with PPE provision undermined the care
system in both nursing homes and in the community. There were issues around people refusing
home care services due to concern that home care workers would bring the infection into their
home. The inability of Government to find a solution to the child-care needs of frontline health and
social care staff (mostly women) exacerbated their already very stressful situation.
Safeguarding issues
Throughout the pandemic, nursing home residents experienced significant isolation which affected
their mental well-being. Many reported, particularly during the first and second lock downs of being
confined to their rooms without any interaction with other residents, who were their friends,
leading to feelings of loneliness and distress.
In a general way it is reasonable to state that people in nursing homes were at greater of getting
Covid. There was a significant safeguarding issue here in that some vulnerable adults did not need to
be in nursing homes and were only there because of inadequate home care supports.
It is also the case that some people living at home were more at risk because of the absence to a
large extent of any outside people coming into the home and the pressures on relatives who were
not used to providing high levels of care for loved ones. This was seen as especially relevant where
families were taking on additional caring roles and where there was less engagement by outside
professionals and more involvement by volunteers not all of whom would have gone through a
vetting process. It was also the case that HSE Safeguarding and Protection Teams only had skeletal
staff available (e.g., one social worker in each county) and could not adequately respond to the high
number of concerns being reported.
End-of-life care in nursing homes
End-of-life care in nursing homes presented additional difficulties during Covid-19 especially in
relation to relatives not being able to visit. This was particularly difficult for families who were not
able to have quality time with a loved one who was dying but who did not have Covid-19. Some
families expressed concern to Sage advocates about how well pain was managed when they were
not able to be present to monitor it. There was also a total lack of clarity for relatives as to what was
permitted in terms of being with a loved one at end of life.
The following are some other general observations based on the Sage Advocacy experience:
– It is clear that that preparation by the nursing home sector (public and private) for what was
well known at the outset to be a very infectious disease was inadequate.
– The fact that the HSE did not have a direct relationship with private nursing homes was a
matter of huge concern which needs to be addressed.
– There was a significant underestimation of the potential effects of Covid-19 on nursing home
residents with the primary focus on ensuring that acute hospitals would be able to cope.
– Concerns were identified in respect of vulnerable adults who were at home with family
members full-time where there was no external oversight and which could potentially give
rise to safeguarding issues.
– Some people were discharged to a home environment that was not conducive to their care
in that their family was not supportive because they feared that this arrangement would
become long-term and that they could not sustain it.
– The lack of childcare for essential health care workers was identified as an ongoing issue
which resulted in some people having to opt out of essential frontline work.
– There were situations reported where family members had asked the home carers to cease
visiting without any consultation with the older person who was the care recipient.
– The isolation, lack of physical contact with relatives and friends, coupled with fear and
anxiety almost certainly impacted on the mental health and well-being of many nursing
home residents.
– The fact that most medical appointments were cancelled or suspended, e.g. cancer
treatments, diabetic retinopathy, rheumatology was regarded by Sage advocates as having
potential long-term effects on people.
– The understandable fear that people had of going to an acute hospital led to uncertainty and
anxiety as people lived with conditions that they knew required hospital intervention.
How Ireland responded to the Covid-19 crisis: Observations by Sage Advocacy
The focus of the first weeks of the crisis was on sustaining hospitals and ensuring that they would be
able to deal with the pandemic. This challenge was met purposefully and adequately. However, it
quickly became clear that the virus had swiftly taken hold in nursing homes and in other residential
care facilities. This brought into focus the fractured picture of health and social care services, which
range from acute hospitals to large nursing homes, through community support services and
homecare and individuals organising their own support infrastructure. While the freeing up of acute
hospital beds to accommodate Covid-19 cases was deemed necessary at the outset, this resulted in
two negative outcomes; (a) unplanned discharges to nursing homes and to the community; and (b)
the non-availability of other hospital-based medical interventions.
Health and social care services faced unprecedented pressures and there was a necessary and
important focus on keeping people safe. As the pandemic progressed, it became increasingly clear
that nursing homes, particularly private nursing homes, were not managing the challenge posed by
Covid-19. The State, while slow to respond initially, did put in place a number of important
mechanisms10 which helped to address the situation including, in particular:
– Enhanced HSE engagement with the private nursing home sector
– Temporary HSE governance arrangements for some non-public nursing homes
– Multidisciplinary clinical supports at CHO level through Covid-19 Response Teams
– Access to supply lines for PPE, Oxygen etc.
– Access to staff from community and acute hospitals
– Temporary financial support scheme
– HIQA Infection Prevention Hub and
– Covid-19 quality assurance regulatory framework
In effect, the HSE moved from a position whereby the private nursing home sector (which was seen
as an entirely separate system made of up of individual private entities (albeit with a statutory
funding stream and regulated by HIQA) to a position whereby the HSE provided a significant level of
support both nationally and locally in response to the crisis.
HIQA eventually established a range of contingencies and measures to ensure ongoing remote
assessment of services and developed a quality assessment process whereby all designated centres
were formally contacted on a fortnightly basis by an inspector of social services to assess how they
were coping, and any deficits identified in their ability to sustain a safe, high-quality service.
Critical overarching matters
While the freeing up of acute hospital beds to accommodate Covid-19 cases was deemed necessary
at the outset, this resulted in two negative outcomes; (a) unplanned discharges to nursing homes
and to the community; and (b) the non-availability of other hospital-based medical interventions.
The closure of specialised units in some hospitals (e.g. rheumatology) to accommodate anticipated
high numbers of Covid patients, undoubtedly, had adverse effects on people with some conditions.
To date this is a matter that has not got the attention that it warrants. Sage Advocacy believes that it
should be addressed as a matter of importance by the Covid-19 Evaluation Team.
Sage Advocacy believes that home care providers, regardless of whether HSE or private, should
have been able to assure families that they could meet all the safety and PPE recommendations –
this did not happen in an adequate manner.
Focus on over-70s
The singling out of over-70s by Government for particular attention and restrictions was
discriminatory and ageist, especially as the message put out there clearly implied that travel
restrictions and cocooning was a legal requirement rather than guidance.
The Government passed the Health (Preservation and Protection and other Emergency Measures in
the Public Interest) Act 2020, which contained provisions to fine or imprison those who do not obey
an order from a garda if that garda believes the person is making an unnecessary journey outside a
2km zone from their home.
While there was no provision in the Act to sanction those that ought to be cocooning and were not,
many people believed it was illegal to go out if they were over 70. This undoubtedly resulted in
confusion, annoyance and a rightful feeling on the part of many older persons that they were being
discriminated against.
It goes without saying that most people over the age of 70 are fit and healthy and would have had a
pre-existing lifestyle of active exercise and active participation in society, including as volunteers in
delivering a range of social services. The cocooning message from Government sought to limit that.
Also, the prolonged nature of the cocooning undoubtedly took its toll on some older people’s wellbeing and mental health.
Data on deaths from Covid
Another hugely important matter is the fact that the death of any person who had Covid was reported
as a Covid death. The fact that a person with Covid could have died because of some other reason or
multiple other reasons was ignored in the reporting of numbers of Covid deaths. This was essentially
disinformation by Government in that it was deliberate rather than inadvertent and, as such, was
essentially unethical. The public, and particularly those at greater risk of Covid and their families had a
basic right to be told the truth.
Key considerations for the future
Arising from the foregoing, Sage Advocacy identifies some important factors that need to be
acknowledged and reflected in future responses to any major crisis in health care:
✓ The blurring of the boundary between legal requirements and public health guidance should not
have taken place from either a human or a legal rights perspective.
✓ The lack of human rights and equality expertise in the decision-making structures put in place
relating to Covid-19 was a significant omission.
✓ Generic policy responses failed to take account of the additional and specific needs of different
population cohorts with reference to older persons living alone, in nursing homes or in isolated
communities;
✓ Due to their vulnerability to the virus and the impact of public health measures such as
‘cocooning’, older people experienced a significant level of isolation and dislocation from their
families, and prolonged disconnection from social supports.
✓ There was insufficient focus in the policy response on the need to balance the requirement to
protect health and life with other important rights and freedoms.
✓ On a more general level, people who did not have access to technology (the digitally excluded),
many of whom would have been older persons, were disproportionately affected by the focus
on remote/virtual communication, adding another layer of discrimination.
As a general observation, the need for new models of nursing home care and for an integrated
continuum of support and care came starkly into focus because of the pandemic experience. The
important point has been made that living in nursing homes makes it intrinsically difficult to
physically distance oneself and that “living with any concentration of people categorised as
‘vulnerable’ to the disease [Covid-19] was a disaster waiting to happen.11 This point is all the more
pertinent because there is a relatively high proportion of people currently in nursing homes who
would not be there if a an adequate home care support infrastructure was in place.
A centrally important question that needs to be addressed by the Covid Evaluation Team is what
additional HSE and HIQA inputs will be required on an ongoing basis to prevent the dismal scenario
that emerged in nursing homes and how the positive aspects of the crisis-based interventions put in
place can be consolidated and sustained in the longer-term.
Some of the following information has been redacted for GDPR purposes.

Footnote
(1 Sage Advocacy notes that there will be further consultation by the Evaluation Team relating specifically to
nursing homes.)
2 https://data.oireachtas.ie/ie/oireachtas/committee/dail/33/special committee on covid19_response/reports/2020/2020-07-31_interim-report-on-covid-19-in-nursing-homes_en.pdf
3 https://www.gov.ie/en/publication/3af5a-covid-19-nursing-homes-expert-panel-final-report/
4 https://www.hiqa.ie/sites/default/files/2020-07/The-impact-of-COVID-19-on-nursing-homes-in-Ireland_0.pdf
5 http://dementia.ie/images/uploads/site-images/DSIDCReport_439721.pdf
6 https://www.hiqa.ie/sites/default/files/2020-04/Assessment-framework-DCOP-covid19-preparedness.pdf
7 https://data.oireachtas.ie/ie/oireachtas/debateRecord/special_committee_on_covid-19_response/2020-05-
26/debate/mul@/main.pdf
8
https://data.oireachtas.ie/ie/oireachtas/committee/dail/33/special committee on covid19_response/reports/2020/2020-07-31_interim-report-on-covid-19-in-nursing-homes_en.pdf
9
https://www.npr.org/sections/health-shots/2020/04/21/838794281/study-raises-questions-about-falsenegatives-from-quick-covid-19-test?t=1594981639899
10 file:///C:/Users/Cloon/Downloads/74796_d09c1f51-435f-4b73-9433-923ce3d531f9%20(5).pdf
11 G. Quinn and A. Campbell https://www.irishtimes.com/opinion/nursing-homes-must-be-made-a-thing-ofthe-past-1.4257422