Introduction
The Irish Nurses and Midwives Organisation (INMO), representing the majority of nurses and midwives across Ireland in both the public and private sectors, welcomes the opportunity to contribute to the COVID-19 Evaluation.
Although Ireland did not experience excess mortality rates, the impact of the pandemic was far-reaching. It remains essential to critically reflect on the pandemic, its effect on the country, and the effectiveness of the national response.
This submission centres on the vital issue of protecting nurses and midwives during the COVID-19 pandemic and outlines key reforms needed to strengthen preparedness and resilience in future public health emergencies.
Pandemic Preparedness – Legacy Challenges
Underfunded Healthcare Service
Decades of underinvestment and piecemeal reform have left the Irish healthcare service vulnerable, overstretched, and ill-equipped to cope with the demands placed upon it, which impacted the ability of the health service in its response to the COVID-19 pandemic.
The pandemic exposed the cumulative consequences of failing to adequately fund and reform healthcare. Numerous reports highlighting staff shortages and infrastructural deficits were published over the years, yet successive governments and the HSE failed to act. As a result, Ireland entered the pandemic with a health system lacking the resilience and surge capacity required to respond effectively.
Recommendation: The Government must commit to multi-annual public health service funding to ensure continuity of care and build system capacity to respond to future public health emergencies as recommended by the Public Health Reform Expert Advisory Group.
Health Service Capacity
Ireland’s acute hospital system has operated at dangerously high occupancy rates for years. The OECD reports that Irish acute beds are occupied at a rate of 95%, well above the recommended safe threshold of 80%.
Primary and community care services, vital to easing pressure on the acute sector, were significantly underdeveloped pre-pandemic. The long-standing failure to invest in these areas hindered the full implementation of Sláintecare and compromised efforts to shift care into the community.
The recently published ESRI (2025) report shows that population growth, demographic ageing, and the legacy of the pandemic have significantly altered demand projections. Demand for care is now expected to rise by 40% by 2040, exceeding previous forecasts.
Timely discharge from acute hospitals also remains a significant challenge. There is an urgent need for additional transitional and step-down care beds to relieve congestion in acute settings.
The pandemic also underscored the importance of adaptable and scalable bed capacity, particularly in critical care units. The INMO welcomes the recommendation from the ESRI to commence a national projection exercise on CCU/ICU capacity to prepare for future surges in demand.
It must also be acknowledged that poor working conditions and environments directly impact the wellbeing of nurses and midwives and patient outcomes. Working in persistently overcrowded, understaffed, and high-pressure settings cannot be accepted as the norm. The HSE, as the employer, holds a responsibility to provide safe, supportive, and adequately resourced work environments that promote high quality care and staff retention. This includes ensuring appropriate staffing levels, safe skill mix, and physical conditions that allow nurses and midwives to carry out their roles effectively and safely.
Recommendation: There must be strict adherence to 85% occupancy of acute hospitals and zero tolerance of hospital and emergency department overcrowding.
A national projection exercise on CCU/ICU bed capacity is required to prepare for future public health emergencies.
Universal Healthcare (UHC)
Ireland continues to stand out as an outlier among high-income countries due to the absence of a universal healthcare system. This concern was reinforced by the WHO’s (2023) review of Ireland’s delivery of Essential Public Health Functions (EPHF) post pandemic, which identified the over-reliance on acute healthcare services as a key systemic shortcoming.
The principles underpinning Sláintecare remain more relevant than ever. The goal of establishing a universal, single-tier health service must be fully realised, where access is based on health need and not ability to pay.
The fragmented nature of Irish healthcare delivery has deepened inequalities and weakened system-wide coordination. The lack of reform progress, particularly in community-based services and integrated care pathways, has hindered the delivery of seamless, equitable care. Chronic underfunding of primary care and community health care services contradicts the vision of Sláintecare and continues to unnecessarily push patients into acute hospitals.
If Ireland is to realise UHC in practice, it must be underpinned by legislation, adequate staffing and sustainable funding. Sláintecare cannot be delivered without the nursing and midwifery workforce being recognised, valued, and resourced to lead on integrated and nurse-led models of care.
Recommendation: Accelerate the implementation of Sláintecare to establish a universal healthcare system, underpinned by sustained investment in primary and community care services. This must include appropriate workforce planning and funding to ensure adequate nurse and midwife staffing across all settings.
Safe Nurse and Midwife Staffing
Workforce planning failures, staffing deficits, and a growing mismatch between demand and capacity have consistently hampered the Irish healthcare system. These longstanding issues were magnified during the pandemic, creating unsafe conditions for both patients and staff.
The recruitment pause/freeze of 2007 placed immense pressure on an already struggling workforce. Subsequent recruitment freezes further exacerbated these staffing shortages. The continued failure to implement and fully fund a workforce plan, including robust recruitment and retention strategies, has significantly contributed to the persistent staffing challenges faced by the health service.
Workforce sustainability was further threatened by demographic changes, with both the patient population and the nursing/midwifery workforce ageing. Amid rising comorbidities, increasing care complexity, and a low domestic supply of nurses and midwives, urgent and sustained action is needed to attract, retain, and support the nursing and midwifery workforce.
The Framework for Safe Nurse Staffing and Skill Mix has proven effective in improving outcomes, reducing adverse events, and supporting staff retention. However, its full implementation is now urgently required across all healthcare settings.
Similarly, in maternity care, the full funding and implementation of the National Maternity Strategy is essential to ensure safe, high-quality services. The Strategy’s recommended midwife-to-birth ratio of 1:29.5 remains unimplemented, jeopardising maternity safety.
Furthermore, the Birthrate Plus tool should be mandated to determine appropriate staffing levels across all services. Legislation must underpin the requirement to maintain safe staffing levels, ensuring consistent and reliable care.
Safe staffing must become a legal requirement. The Patient Safety (Licensing) Bill provides an opportunity to enshrine safe nurse and midwife staffing levels in legislation. Doing so would protect patient safety, improve quality of care, and help reduce costs over the long term.
Recommendation:
- Fully implement the Framework for Safe Nurse Staffing and Skill Mix across all healthcare settings.
- Mandate the use of the Birthrate Plus tool, including the 1:29.5 midwife-to-birth ratio and urgently fund and implement the National Maternity Strategy.
- Enshrine safe nurse and midwife staffing levels in legislation through the Patient Safety (Licensing) Bill.
Future Pandemic Preparedness
The INMO welcomes Ireland’s commitment to implement the WHO’s International Pandemic Agreement (WHO, 2025). This is crucial in planning for future public health emergencies and pandemics.
Article 7 of the agreement focuses on the health and care workforce and identifies several obligations for the Irish Government going beyond immediate responses to a potential pandemic. Indeed, many of these issues are significant challenges for the public health system.
A key area for the Government will be to ensure that it takes appropriate action to “develop, strengthen, protect, safeguard, retain and invest in a multidisciplinary, skilled, adequate, trained, domestic health and care workforce to prevent, prepare for and respond to health emergencies”.
Article 7, point 2 explicitly places an obligation on the Government to ensure decent work for HCWs and protections to ensure “the continued safety, mental health, well-being, and strengthen capacity of its health and care workforce”.
Therefore, the highest form of protection must be afforded to nurses, midwives and other HCWs working across the health service.
Recommedation: Ireland must prepare for future public health emergencies in line with the WHO International Pandemic Agreement
Nursing and Midwifery Leadership
Post pandemic, a key recommendation from the WHO/WHPA (2022) is to “bolster the role of HCWs in leadership and decision-making levels” to ensure appropriate protections and acknowledgement of the risks of working in the health and social care.
Nurses and midwives are integral to strengthening health systems, building community resilience, and maintaining essential health services during times of crisis. Their leadership in emergency preparedness and response enables health services to adapt rapidly, minimise disruption, and safeguard both patient outcomes and the quality of care (WHO, 2025). Given this, their expertise and leadership must be at the core of Ireland’s pandemic preparedness efforts, with a meaningful role in strategic planning and key decision-making processes.
However, key opportunities were missed during the pandemic to fully integrate nurses and midwives into Ireland’s pandemic response, despite these professions making up approximately one-third of the healthcare workforce.
Notably, it took an entire year before the Chief Nursing Officer (CNO) was appointed to the membership of NPHET. Similarly, when the COVID-19 Advisory Group was established, the absence of a nurse or midwife among its members drew strong criticism from the INMO.
Excluding nursing and midwifery from such critical advisory bodies reflected a disconnected and unrealistic approach to pandemic planning that overlooked the lived realities and frontline expertise within the health service.
These omissions resulted in a significant loss of insight and leadership at the decision-making table, ultimately undermining the nursing and midwifery contribution and professional standing during a national crisis.
Recommendation: Ensure nursing and midwifery leaders are appointed to all pandemic preparedness and response national and regional committees to ensure their expertise informs planning, decision-making, and frontline service delivery.
The Role and Impact of Nurses and Midwives During the COVID-19 Pandemic
It is essential to begin by acknowledging and sincerely thanking the nurses and midwives of Ireland for their unwavering dedication, extraordinary commitment, and compassion throughout the COVID-19 pandemic often at risk to themselves or their loved ones. From the earliest days of the crisis, they stood on the frontlines of the health service, adapting, leading, and responding to ever-evolving challenges with professionalism, resilience, and clinical expertise. Their courage and selflessness must be formally recognised and never forgotten.
Redeployment and Reskilling
The nursing and midwifery workforce demonstrated remarkable agility through widespread redeployment during the pandemic. Nurses and midwives were reassigned to many areas, including intensive and critical care units (ICUs/CCUs), private residential care facilities, infection prevention and control, testing and tracing teams, and vaccination centres.
For example, Ireland’s critical care capacity increased by 75% during the second wave of the pandemic, enabled primarily by the redeployment and reskilling of nursing staff (Department of Health, 2020).
It must be noted that redeployment was not always straightforward and came with challenges for staff. Such transitions often required rapid upskilling, further highlighting the dedication and professionalism of the workforce in the face of unprecedented pressures.
Flexibility and Adaptation in Care Delivery
Nurses and midwives rapidly adjusted their practice throughout the pandemic to meet urgent and changing needs. Delivering care in both COVID and non-COVID environments, the patient was kept central to their work. They developed and implemented new models of care and redefined patient care pathways to ensure safe and effective care. (O’Regan-Hyde et al., 2024).
For example, in maternity services, midwives ensured that care for women and infants continued to the highest standards despite evolving restrictions. Public health and community nurses restructured their heavy caseloads and care delivery to support isolated COVID-19 patients and the continuation of regular services (Department of Health, 2020). Registered Nurses in Intellectual Disability (RNIDs) continued to provide essential advocacy and care for people with intellectual disabilities, despite the challenges posed by strict public health measures.
The pandemic accelerated the development of new care models and work practices. Nurses and midwives led the rollout of telehealth clinics, particularly in outpatient and community settings. In May 2020 alone, over 85,000 outpatient appointments were conducted virtually, helping to maintain continuity of care while reducing the risk of hospital-acquired infections. Such innovations have the potential for long-term positive transformation of the healthcare system.
Vaccination and Testing
Nurses and midwives played an essential role in Ireland’s COVID-19 vaccination programme. Drawing on their long-standing involvement in immunisation, many were redeployed or postponed retirement to support vaccine delivery, with others volunteering for frontline roles. On 29 December 2020, a nurse administered Ireland’s first COVID-19 vaccine, marking a historic day for the country. Nursing and midwifery professionals also led key operational and leadership roles in the national test and trace programme, contributing significantly to its rapid expansion.
Leadership at All Levels
Nurses and midwives consistently demonstrated leadership throughout the crisis, both in patient-facing roles and at strategic levels. They were represented on numerous national forums and taskforces, including the National Vaccine Taskforce, the Clinical Placement Oversight Group, and the Vaccination Clinical Support Group (Department of Health, 2022). Their leadership helped shape national responses and policies, reinforcing their essential role in Ireland’s healthcare system.
Recommendation: The COVID-19 Evaluation must formally recognise the extraordinary commitment, professionalism and leadership of nurses and midwives during the pandemic.
Physical and Psychological Impact on Nurses and Midwives
The COVID-19 pandemic had a profound impact on nurses and midwives. INMO members worked tirelessly to deliver high-quality, safe patient care under exceptionally challenging conditions. While the professions are well accustomed to working under pressure, the pandemic imposed unprecedented demands.
In a 2020 INMO survey, members highlighted physical exhaustion due to heavy workloads, staffing shortages, and redeployment. Many also reported significant fatigue, particularly from the prolonged use of PPE:
“Working for hours upon hours in PPE was exhausting. I worked in an acute geriatric ward, many of which need help washing, dressing, hoisting, falls risk, PPE gear had to be worn for long periods of time often making my colleagues in I feel physically sick with the heat and constant physical demands.”
“Physical exhaustion working extra shift trying to maintain safe staffing levels” “I have never in my 30+ years nursing experienced such fatigue. My colleagues hospital wide have similar stories of headaches and exhaustion and low energy and lethargy.”
The ICN has described the experience of nurses and midwives during the pandemic as “mass traumatisation of nurses worldwide” (ICN, 2021). The INMO undertook several surveys of its members during the pandemic. All have provided evidence of nurses and midwives under immense pressure, experiencing exhaustion and concern for their mental health.
The following data was extracted from surveys exploring the psychological impact of COVID-19. The results describe how respondents expressed increased consideration for leaving the profession, increased mental exhaustion and worry for their personal health during the pandemic.
| Psychological Impact of COVID-19 Surveys | 2020 | 2021 |
| Has your experience of working during the COVID-19 caused you to consider leaving the profession? | Yes 61.02% | Yes 68.33% |
| Do you believe that your experience of COVID-19 has had a negative psychological impact on you? | Yes 82.71% | Yes 84.89% |
| When off duty, have you experienced any of the following since the COVID-19 pandemic? Mental Exhaustion | Yes 90% | Yes 98.48% |
| I feel that my personal health has been put at risk | Strongly Agree or Agree 83% | Strongly Agree or Agree 84.45% |
Burnout is an increasingly prevalent issue amongst nurses, midwives and other healthcare workers, exacerbated during the pandemic. (O’Brien, 2024). Mental exhaustion is one of the core components of burnout; the survey found that more than 90% of nurses and midwives reported being mentally exhausted (INMO, 2020; 2021).
Similarly, many respondents reported evidence of burnout in the qualitative responses:
“I am currently on sick leave with burnout.”
“Severe burnout with no light at the end of the tunnel. Very disappointed with how nurses have been treated by our supposed caring health service.”
“At this stage of the pandemic, it feels like a complete burnout”
“Have suffered with burnout, stress and anxiety requiring medication and time off work to assistme through COVID period of which this is still an ongoing concern.”
“I feel so burnt out as a student nurse, I feel very low.”
“Successful public health outcomes are hugely contingent on the effective functioning of the workforce.” (Gavin et al., 2020). Protecting the mental health of HCWs was identified early in the pandemic as a global priority by the WHO, intrinsically linking patient outcomes to the wellbeing of nurses and midwives. This was strongly echoed by international and national nursing and midwifery bodies (RCM, 2020; ICN, 2021; WHO Europe, 2022; WISH, 2022). WHO Europe’s (2022) post-COVID workforce recommendations emphasised the need to “protect the health and mental well-being of the workforce.” This principle must underpin all efforts to support nurses and midwives across every healthcare setting, both now and into the future.
The International Labour Organization’s (ILO’s) Biological Hazards in the Working Environment Convention, 2025 (No. 192) has further underscored the equal importance of safeguarding both the mental and physical health of workers.
Although the acute phase of the pandemic has passed, its psychological and physical impact on nurses and midwives remains significant and may continue to affect workforce retention, resilience, and sustainability if not adequately addressed.
Recommendation: A national occupational health service, inclusive of all healthcare settings, must be developed and resourced to support the physical and mental health needs of nurses, midwives and other healthcare workers.
Government Response – Precautionary principle
While the COVID-19 pandemic presented an unprecedented public health challenge, the response to the evolving crisis, particularly as more infectious variants emerged, was often too slow to protect those on the frontline adequately.
The systems in place at the time were overly complex, involving multiple agencies, including NPHET, the HPSC, and the HSE, and this fragmentation frequently left nurses and midwives sidelined in the decision-making process. Significant delays in updating and implementing policies led to repeated and avoidable exposure of frontline staff and patients to infection risks.
Whether in providing PPE, managing HCW infections, addressing hospital overcrowding, or ensuring safe working conditions, at nearly every stage, the precautionary principle was not adequately applied.
Rather than prioritising maximum protection until the science became clearer, responses were often reactive and inconsistent.
On behalf of our members, we had to advocate for the most basic safety measures from the outset. A public campaign had to be launched simply to secure face masks. Even essential supports, such as childcare for the predominantly female healthcare workforce, were overlooked when schools closed.
These shortcomings reflected a broader failure to centre HCW safety in the national response. A clear, consistent message valuing and protecting frontline staff was missing at critical moments, often when it mattered most.
Recommendation: Apply the precautionary principle as a core standard in all future public health emergencies by prioritising the safety of HCWs from the outset.
High Healthcare Worker Infection Rates
The impact of COVID-19 was profound, and tragically, according to the HPSC (2024), 23 HCWs in Ireland lost their lives (01/03/2020 to 06/01/2024). Their deaths are a stark reminder of the risks faced by those on the frontline and of the ultimate sacrifice.
HCWs were consistently among the most exposed occupational groups throughout the pandemic. As of 13 November 2023, a total of 100,409 HCWs in Ireland had been infected with COVID-19.
During the first wave, nurses and midwives, in particular, experienced unprecedented levels of infection. Figure 1 illustrates the disproportionate burden of COVID-19 cases among HCWs compared to the general population between March and June 2020.
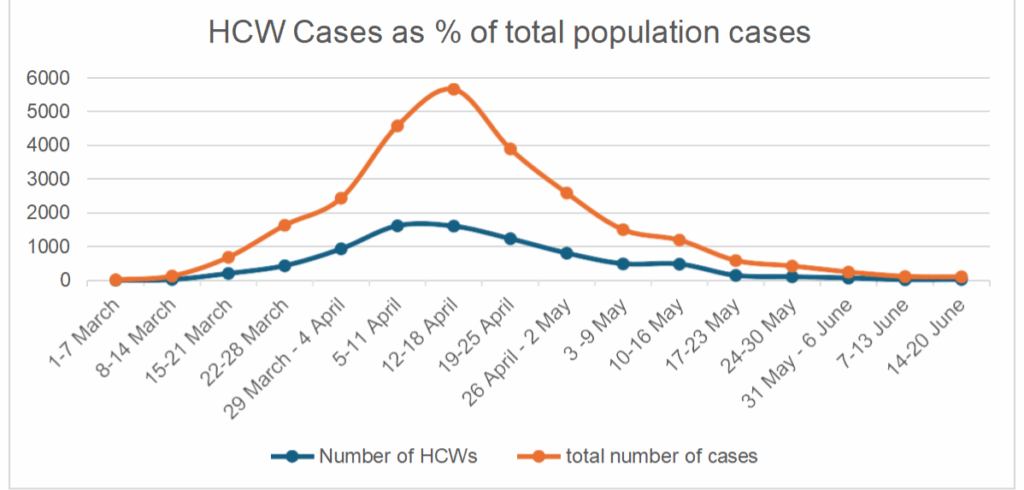
Figure 1 – HCWs as % of total population cases
The Prevalence of Antibodies to SARS-CoV-2 in Irish Healthcare Workers: Phase 1 Interim Report (HPSC, 2021) further highlighted the heightened vulnerability of specific roles within the sector, identifying nurses, midwives, and healthcare assistants (HCAs) as being at the greatest risk of exposure and infection.
Data from the HPSC (2020) further supports this, showing that as of 29 June 2020, HCWs accounted for 31.9% of all confirmed COVID-19 cases in the population. Within this group, nurses, midwives, and HCAs comprised nearly 60% of all healthcare worker infections. Significantly, nurses and midwives alone represented 10.43% of the total confirmed COVID-19 cases nationally, a stark indicator of the disproportionate impact on these frontline professionals.
| Total population cases | Nurses | Health Care Assistants (HCAs) | Other HCWs | |
| As at 29 June | 25,874 | 2,700 | 2,149 | 3,411 |
| % of the total population | 100% | 10.43% | 8.30% | 13.18% |
Table 1 – COVID-19 cases in HCWs
Globally, the International Council of Nurses (ICN) (2020) collected data on COVID-19 infections among HCWs from over 30 countries, comparing HCW infections as a proportion of total national cases. While differing definitions and reporting practices complicate international comparisons, such data remain critical for informing infection prevention and control (IPC) strategies and protecting HCWs. The ICN found significant variation across countries:
- Less than 1% in Singapore
- 12% in Italy
- 15% in Mexico
- 22% in Spain
According to the ICN, Ireland had the highest known proportion of HCW infections at 32% at this time.
While infection rates declined in later waves, the proportion of HCWs infected remained high, with spikes at various times. This affected the personal well-being of healthcare staff and placed considerable strain on healthcare service delivery.
In our view, the infection rate among Irish HCWs was disproportionately high compared to the general population, and key interventions could have reduced this burden.
The INMO consistently campaigned on this issue, raising serious concerns with the Minister for Health, the Chief Medical Officer, and senior figures in the HSE. We consistently issued public statements throughout the pandemic to hold health service employers more accountable and raise awareness of the profound impact on our members. These communications highlighted the unacceptable risks faced by HCWs, calling for independent scrutiny into the high rate of infections. (PR: Rapid, independent inquiry into healthcare worker infection needed, Saturday 30 May 2020; PR: Majority of recent COVID cases are healthcare workers, Thursday 25 June 2020.
While data on HCW infections is no longer published, the HPSC’s most recent study (2024) highlights the persistent risk of SARS-CoV-2 infection among HCWs in Ireland despite high vaccination rates, prior infection, and widespread seropositivity. Although severe illness was notably absent in HCWs, ongoing infections continue to disrupt healthcare service delivery, particularly during periods of increased respiratory virus circulation, such as winter.
Recommendation: Future pandemic planning must explicitly recognise the disproportionate risk faced by nurses and midwives. Targeted protective measures should be built into occupational health strategies for high-risk healthcare roles.
Infections Acquired in Healthcare Settings
COVID-19 outbreaks posed a significant risk to both patients and HCWs throughout the pandemic and continue to present challenges today.
A survey conducted by the INMO at the onset of the pandemic revealed that 78.49% of respondents feared contracting the virus in their workplace. These concerns were well-founded. During the first wave, healthcare acquired infections among HCWs reached alarming levels. Official figures presented to the INMO showed that, as of 30 May 2020, 88% of infected HCWs had likely acquired the virus in a healthcare setting (INMO, 2020).
While data on healthcare acquired infections was not always available, data from the HPSC, presented in Table 2, provides a sample of healthcare-acquired infections early in the pandemic. It shows that nearly 70% of COVID-19 cases among HCWs during the first wave were likely acquired in a healthcare setting. A further 14.3% of cases remained under investigation regarding their source of transmission.
| Likely source of transmission | Number | Percentage |
| Healthcare setting acquired: staff* | 5,712 | 69.30% |
| Close contact with a known confirmed case | 947 | 11.40% |
| Travel related | 140 | 1.70% |
| Community transmission | 228 | 2.80% |
| Healthcare setting acquired: patient | 50 | 0.60% |
| Under investigation | 1,183 | 14.30% |
| Total | 8,260 | 100% |
Table 2 – Likely source of COVID-19 transmission – Source: Report of the profile of COVID-19 cases in healthcare workers in Ireland Report prepared by HPSC on 29/06/2020.
The INMO consistently raised concerns about healthcare acquired infections throughout the pandemic. Our firm view remains that when a worker contracts an illness in the workplace, each case should be thoroughly investigated to determine how the infection occurred and what measures can be implemented to prevent recurrence.
Recommendation: All cases of healthcare acquired COVID-19 among HCWs must be subject to thorough investigation, with a clear focus on identifying causative factors and implementing preventative measures.
Notification of COVID-19 Cases to the HSA under the Safety, Health and Welfare at Work (Biological Agents) (Amendment) Regulations 2020
In April 2020, amid rising healthcare worker infection rates, the INMO urged the Government to amend health and safety regulations to make COVID-19 a reportable occupational illness. We also called on the HSA to mandate formal reporting of all occupationally acquired cases, highlighting the need for accurate data, accountability and effective prevention measures (Ref: Letter to Sharon McGuinness, Re: Return to Work Safely Protocol, 15 May 2020).
Although the Government had the authority to act, it took no steps until required by law. Despite early requests from the INMO and ICTU, no action was taken until the EU Biological Hazards Directive 2020 was transposed into Irish law in November 2020 under the Safety, Health and Welfare at Work (Biological Agents) Regulations 2020. These Regulations classified COVID-19 as a biological agent and were accompanied by the 2020 Code of Practice, which requires employers to notify the HSA of confirmed workplace cases. This imposes a duty on the HSA to investigate outbreaks, identify causative factors and review the adequacy of risk assessments.
Prior to this, the Government had relied on the “loophole” in the Safety, Health and Welfare at Work (General Application) Regulations 2016,1 which allowed employers to avoid reporting COVID-19 cases to the HSA, resulting in a lack of independent oversight of workplace safety.
Given the significant number of workplace clusters and outbreaks, independent investigations were critical to identifying whether further control measures were needed. Throughout the pandemic, the INMO consistently pressed the HSA to investigate healthcare-acquired infections and ensure protective measures were implemented. Formal complaints were lodged under the 2005 Act and the 2020 Code of Practice (Ref: Letters to Mr Mark Cullen, HSA, January 2021 and 28 January 2021).
The INMO welcomed the recommendation of the Oireachtas Special Committee on COVID-19 to undertake a comprehensive review of the regulatory frameworks governing the HSA, including the adequacy of its powers and resourcing and believe this should now be progressed.
Ultimately, the delayed response by the Government to classify COVID-19 as a reportable occupational hazard represented a missed opportunity to protect HCWs proactively. The necessary regulatory amendments took place only when legally compelled by European legislation, despite early and repeated calls from the INMO and ICTU.
Recommendation: In future public health emergencies, Irish health and safety legislation must evlove and be fully implemented to reflect the significant risks faced by healthcare workers, with a clear legal obligation on employers to protect their staff.
Healthcare Worker Surveillance
While we acknowledge that the HPSC published basic data on HCW COVID-19 infections, concerns arose regarding the consistency, level of detail and timeliness of this reporting.
It initially took considerable time for data to become available. Although the INMO consistently campaigned for more comprehensive data, including healthcare acquired infections, outbreak settings, and close contact details, the only data consistently published was the overall number of HCWs who tested positive.
Such data is fundamental to understanding how COVID-19 was impacting nurses and midwives. Therefore, the INMO raised these concerns repeatedly with the HSE, the HPSC, and the Minister for Health and highlighted the need for robust, transparent data in a submission to the Oireachtas Special Committee on COVID-19 (July 2020).
Despite these efforts, challenges in accessing adequate and detailed data on HCW infections persisted throughout the pandemic. At several points, reporting was either abruptly discontinued or significantly altered. For instance, the HPSC initially published a detailed HCW report containing valuable information on the profile of infections. However, this report was later reduced in scope, omitting key data. The INMO formally raised concerns regarding these changes in correspondence, including letters to Dr Colm Henry, Chief Clinical Officer, and Dr John Cuddihy, Interim Director (Ref: 5 November 2020; 21 January 2021; 22 July 2022).
The ICN (2020) called for countries to implement standardised data collection on HCW infections and deaths. This included consistent reporting of variables such as occupation, age, sex, ethnicity, underlying health conditions, and outbreak settings. Such data is essential for informing responses that protect both healthcare workers and patients.
Recommendation: There is a critical need for transparent, consistent, and detailed data collection and reporting on HCW healthcare acquired infections/illness/injuries to inform timely decision-making and protect HCWs in future public health emergencies.
Infection Prevention and Control (IPC) Guidance
Infection prevention and control (IPC) is a practical, evidence-based approach designed to protect patients and HCWs from avoidable infections. Throughout the various stages of the pandemic, IPC guidance adapted globally and nationally in response to emerging evidence, adapting strategies to better mitigate risks and enhance safety measures.
Acknowledging the rapidly evolving nature of the pathogen at various stages and the need to ensure evidence-based practices, the INMO believes that specific key IPC preventative measures were not always implemented in a timely manner, acknowledging the precautionary principle.
Personal Protective Equipment (PPE)
PPE was and remains central to HCWs ability to protect themselves and the people in their care across all settings, COVID and non-COVID alike. It is critically important that the most appropriate levels of PPE are consistently available and accessible across the entire health service, including primary, community, voluntary, and private sectors.
Notwithstanding many of the challenges around the supply of PPE, the INMO repeatedly advocated for our members in terms of the requirement for appropriate PPE. An INMO survey (2020) revealed widespread frustration among members regarding the lack of timely and appropriate guidance. Members reported:
“It took too long for wearing of masks to be advised. Many staff would not have been infected if masks were worn earlier.”
“It should have been mandatory for us to be wearing masks from the beginning. The HSE failed in their duty of care to healthcare workers, which resulted in the high numbers of HCWs being infected with the virus.”
Throughout this period, the INMO issued several formal communications to the HSE, calling for a universal mask-wearing policy across all healthcare settings, including maternity and community services, as well as the use of FFP2 masks as recommended by the ECDC (Letters to Dr Colm Henry Chief Clinical Officer, Re: issues and Concerns raise by INMO members, 29 March 2020; Re: Community Nursing Services, 30 March 2020).
In April 2020, the INMO publicly called for updated PPE guidance and improved occupational health policies to ensure HCWs had appropriate time and conditions for self-isolation (PR: 1 in 10 COVID cases are nurses, 17 April 2020). The INMO was forced to initiate a public campaign to demand the introduction of basic facemasks across healthcare settings. While ultimately successful, this campaign reflected our members’ deep frustration that such a fundamental measure required public pressure (PR: INMO welcomes new universal facemask policy across health service, 22 April 2020).
As infection rates surged again in early 2021 and the HSE guidance downgraded the use of FFP2 masks in all settings, the INMO called for national re-implementation of FFP2 respirator masks, citing outbreaks that infected 2,000 HCWs in a two-week period, directly traced to their workplaces (PR: INMO Executive calls for five-point ‘emergency government intervention’, 13 January 2021; PR: Hospital infection rates’ out of control’ – INMO demands strict new measures, 23 January 2021).
Once again, the INMO had to fight for the provision of FFP2 masks, widely acknowledged as international best practice, as the most appropriate protective equipment given the airborne nature of the pathogen. Even after the agreement was reached, it took a month before policy changes were translated into staff access.
In February 2022, the mask mandate was lifted at a time when hospital overcrowding was once again becoming a serious concern. Following the removal of the mandate on 28 February, over 10,000 patients had been left without a hospital bed, and more than 1,600 patients were in hospital with COVID-19.
Together with the Irish Association for Emergency Medicine (IAEM), we called on the Government to take urgent action to curb the spread of COVID-19. Rising infection rates were driving increased hospital admissions, placing immense pressure on already overstretched hospitals and HCWs. (PR: Public health measures needed as a matter of urgency – INMO & IAEM, Thursday 31 March 2022).
It must be acknowledged that a particularly alarming issue was the threat of disciplinary action against nurses and midwives who sought to protect themselves by wearing masks. An INMO survey in 2020 reported:
“Staff wanted to wear face masks earlier, but management threatened disciplinary action.”
“When we wanted to wear surgical masks, we were threatened with disciplinary action.”
Similar threats persisted into 2021 and 2022. Hospital staff in Limerick, Ennis, Nenagh, and Croom were warned they could face disciplinary measures if they independently upgraded to safer PPE (PR: Healthcare staff in Limerick ‘outraged’ at PPE restrictions, 20 January 2021; INMO Opening Statement to Oireachtas Health Committee, 2021; Leahy, 2022).
Such treatment of nurses, midwives, and other HCWs, who sought only to protect themselves and their patients, was wholly unacceptable and contrary to fundamental occupational health and safety principles.
Recommendation: During any future pandemic, all HCWs must be provided with access to the highest standard of evidence-based PPE appropriate to the level of risk. Employers must support, not penalise, staff who take reasonable steps to enhance their own protection, in line with the precautionary principle and health and safety legislation.
Vaccinations
The INMO was critical of the initial rollout of vaccinations for HCWs as it commenced. From the outset, the INMO had consistently warned that HCWs and residents of long-term care facilities must remain the highest priority groups for vaccination. (PR: Healthcare worker vaccination priority must not be overtaken – INMO, Saturday 16 January 2021).
Throughout the early stages of the vaccine rollout, many frontline nurses working in COVID wards and ICUs had still not received their first dose, while non-frontline staff had already been vaccinated. (Opening Statement to the Joint Committee on Health – Protection and Support for Frontline Healthcare Workers, 9 February 2021).
Later in the pandemic, in response to reports that the National Immunisation Advisory Committee (NIAC) had not recommended booster shots for HCWs at that time, the INMO called on the Government to include HCWs in the immediate rollout of the booster programme, framing it as a health and safety imperative. (PR: Government must extend vaccine booster to healthcare workers – INMO, Tuesday 19 October 2021)
Although data was available identifying where the virus was spreading geographically and across the healthcare workforce, this information did not appear to inform the early vaccination strategy. As a result, the vaccine rollout was inconsistent and failed to prioritise areas and workplaces with the highest infection rates, including those adjacent to regions experiencing significant community transmission. Instead, distribution largely followed the HSE’s administrative structures, rather than responding to the epidemiological realities on the ground. This approach lacked appropriate oversight and strategic planning.
The INMO repeatedly raised concerns regarding the lack of planning and sequencing in the initial distribution of vaccines. It was only following engagement with the INMO that sequencing documents were issued to HSE managers on 12th and 19th January. The delay in developing and circulating the Sequencing of COVID-19 Vaccination of Frontline Healthcare Workers document reflects a broader failure to prioritise the protections legally owed to nurses, midwives, and other healthcare workers exposed to COVID-19.
Given the HSE’s statutory duty as an employer to provide a safe place of work, particularly with COVID-19 classified as a biological hazard, such oversight was not only necessary but legally required.
Recommendation: There must be adequate governance, transparency and accountability around vaccination rollout for HCWs. Equally, any agreed list prioritising frontline patient-facing HCWs must not be altered or changed.
Priority Testing for Frontline Workers
Recognising the rapidly evolving nature of the pandemic, particularly in its early stages, the INMO repeatedly called for routine testing and temperature checks for all HCWs, regardless of setting. From early in the pandemic, we believed that the policy of regular testing in residential care facilities needed to be urgently expanded to the acute sector and applied consistently across the wider health service (Submission to the Special Committee on COVID-19 Response: Testing and Contact Tracing, 16 June 2020; PR: INMO to seek urgent meeting with Minister for Health following publication of COVID-19 Nursing Homes Expert Panel, 19 August 2020).
In addition, the INMO requested that the HSE consider introducing antibody testing, particularly in settings with a high incidence of HCW infection. While acknowledging the limitations of antibody testing, we argued that such measures could offer reassurance to staff, particularly where vaccine access had been delayed (Letter to Dr Colm Henry, Chief Clinical Officer, Re: Vaccination and Testing for HCWs, 4 January 2021).
The HPSC’s most recent study (2024) underscores the continued importance of rigorous IPC measures to mitigate exposure and transmission risks in healthcare settings. The authors recommended a role for expanded testing during surge periods due to the high rate of asymptomatic infections.
Protecting HCWs, alongside other high-risk and vulnerable groups, must be central to any future testing and tracing strategy. A long-term, sustainable approach to testing for COVID-19 and emerging pathogens is essential. This requires clear, evidence-based protocols to ensure timely testing, rapid result delivery, and efficient contact tracing. As recommended by the Oireachtas Special Committee on Covid-19 Response, the State should develop a testing and tracing system with a maximum turnaround time of 24 hours, followed by immediate contact tracing.
Recommendation: The Government must establish a permanent, well-resourced testing and contact tracing infrastructure with a 24-hour turnaround target, prioritising healthcare workers and vulnerable populations in all future public health emergencies.
Workplace Policies Occupational Health Supports
The level of occupational support provided to nurses, midwives, and other HCWs during the COVID-19 pandemic was deeply inadequate. Unclear communication regarding occupational health policy changes further exacerbated uncertainty and stress among staff. The INMO consistently raised concerns with the HSE and brought these issues to the attention of several Oireachtas Committees, including the Joint Committee on Health (2021, 2023) and the Special Committee on the COVID-19 Response (2020, 2021).
The WHO Global Health and Care Worker Compact (2023) provides a clear international framework for achieving these aims. The Compact outlines key actions to create safe, inclusive, and dignified working environments, structured around four domains: preventing harm, ensuring inclusivity, providing support, and safeguarding rights. Informed by human rights and international labour law, the Compact offers detailed, practical guidance for governments and employers.
In alignment with these principles, the ILO’s Biological Hazards in the Working Environment Convention, 2025 (No. 192) represents a major advance in international labour standards. It calls on Member States to ensure universal access to occupational health services, with specific emphasis on high-risk sectors such as health and social care. The Convention requires employers to adopt preventive and protective measures in collaboration with workers, and mandates that staff be adequately informed and trained about biological risks. Its accompanying Recommendation offers practical guidance on risk assessments, outbreak response and the development of preparedness systems, all directly relevant to the Irish health service context.
Recommendation: A national occupational health service, inclusive of all healthcare settings, must be developed and resourced to support the physical and mental health needs of nurses, midwives and other healthcare workers.
The Government must also take immediate steps to ratify ILO Convention No. 192 (2025) and incorporate its provisions into national policy, ensuring a robust, rights-based framework to protect the health, safety and dignity of all healthcare workers.
Derogation
The INMO was consistently critical of the HSE’s derogation policy and its subsequent revisions throughout the pandemic.
From the early stages of the pandemic, the INMO called for the reversal of what it viewed as a fundamentally flawed policy. Specifically, the HSE’s approach, allowing asymptomatic healthcare workers who were close contacts to return to work at the discretion of management, was challenged by the INMO on the grounds that it failed to reflect emerging evidence on asymptomatic transmission. In retrospect, this policy decision proved to be a serious error, particularly given the subsequent data on how the virus spread in the absence of symptoms. (Submission to the Special Committee on Covid-19 Response: Infection Risk and Disease in Healthcare Workers; COVID-19 Testing and Surveillance for Healthcare Staff, July 2020).
Concerns regarding the derogation policy were raised regularly by the INMO directly with the HSE, Department of Health, as well as through the National Joint Council (NJC), and formal correspondence was issued on several occasions. (Ref: Letter from Senior ER Executive, Corporate Employee Relations Service, Re: HSE Derogation Policy, 2 October 2020; Letter from NJC to Head of Corporate Employee Relations Services, Re: Healthcare Worker Infection Rates and Derogation Policy, 4 November 2020).
The INMO consistently advocated for the application of the same isolation period of 14 days for healthcare workers as was required under public health guidelines for the general population. We opposed the discretionary shortening of isolation periods for close-contact HCWs, which the derogation policy permitted.
Equally, the INMO was critical of the policy’s monitoring procedures. Although it was confirmed that monitoring mechanisms had only been introduced in the final six weeks of the policy’s use, the INMO remained critical of what was deemed to constitute “monitoring.”
Reports from members indicated that many HCWs were derogated to return to work under a policy that required monitoring measures which were, in practice, neither feasible nor enforceable. In particular, night duty rosters, where managerial oversight was often absent, illustrated the unworkability of the policy. Chronic understaffing further undermined any realistic attempt to monitor health status. Moreover, the only monitoring mechanism consistently reported was temperature checking, which was inadequate to determine whether a close-contact HCW was developing symptoms. (Ref: Letter to Dr Colm Henry, Chief Clinical Officer. Re: Recent Meetings 27 October & 30 October 2020, 5 November 2020).
In 2021, during the third wave of COVID-19, the HSE amended the Derogation Policy to allow HCWs to be exempt from the newly introduced five-day self-isolation rule if a member of their household tested positive for the virus. In our view, this policy revision was a likely factor in reintroducing and spreading the virus within hospitals and other healthcare settings. In response, the NJC wrote to the HSE opposing the policy and raised the matter with the Oireachtas Committee. (Healthcare workers must not be exempt from 5 Day Isolation Rule – INMO, SIPTU, FÓRSA Thursday 18 November 2021; Opening Statement to the Joint Committee on Health Protection and Support for Frontline Healthcare Workers, 2021).
It is the INMO’s view that the Derogation Policy exposed nurses and midwives to an increased risk of infection and likely contributed to the high incidence of COVID-19 among HCWs.
Recommendation: In future public health emergencies, all derogation policies and related workforce practices must adhere to the precautionary principle and align fully with national public health guidance on isolation periods. Protecting nurses, midwives, and other healthcare workers must take precedence over operational convenience.
Childcare
The Government’s failure to provide a workable childcare solution for nurses and midwives as part of the COVID-19 response led to unnecessary pressure on the health service due to reduced numbers of staff available for work. The lack of childcare provision also compounded the nursing and midwifery shortage across the health service.
NERI (2020) highlighted that a lack of childcare disproportionately affects women; 70% of essential workers are female, with over half having children (ESRI, 2020). This reflects the predominantly female nursing and midwifery workforce (96%), many of whom are in childrearing age groups.
During the pandemic, the organisation was received large volumes of communications from nurses and midwives who were deeply frustrated and worried about their childcare situation and how difficult it had become for them.
A survey was undertaken of our members, asking them specific questions relating to their experiences of childcare during the pandemic. The key findings included:
- Almost 60% of respondents stated that they are co-parenting with an essential worker or HCW, resulting in neither parent being available to provide childcare.
- 62% took annual leave to provide childcare.
- 48% of respondent’s spouses/partners took annual leave to provide healthcare.
- Additionally, 30% of respondents took parental leave to provide childcare.
- 38% of respondents experienced difficulty accessing provision of the HSE’s HR
- Circular 033/2020: Working arrangements for those with caring arrangements during COVID-19.
- Over 200 members spontaneously cited stress, anxiety or mental health issues arising from trying to manage childcare.
Such was the fear in the early waves of the pandemic that many respondents reported experiencing social stigma due to their roles as nurses or midwives, with several noting that their children were refused access to childcare services as a result.
Again, the issue regarding childcare was raised through many forums, including a series of correspondence via the NJC (NJC Meeting Summary March – June 2020). In an opening statement to the Oireachtas Special Committee on Covid-19 Response (June 2020), the key issues regarding the lack of childcare were laid out for members. Freedom of Information (FOI) requests made by the INMO to the Department of Health evidence receipt and discussion of regular correspondence between our organsation and the Department in relation to childcare from the outset of this crisis. It also shows that none of our attempts to obtain information received a meaningful response.
The HSE, Department of Health, Department of Youth and Child Affairs, and Department of Expenditure and Reform offered inadequate solutions, ultimately failing the nursing and midwifery professions. FOI communications revealed the HSE deferred to NPHET but remained unwilling to provide clear, supportive measures for their staff, adding confusion and stress during an already challenging time.
Recommendation: A sustainable and responsive, publicly delivered childcare support system must be developed for nurses, midwives and other HCWs, to ensure workforce stability during public health emergencies.
Recognition of COVID-19 as an Occupational Disease
To classify COVID-19 as an occupational disease, a clear link must be established between exposure to the virus and the work environment. Recognising this, the European Commission has formally acknowledged COVID-19 as an occupational disease, specifically highlighting the elevated risk faced by HCWs:
“Healthcare staff are recognised by the European Commission in that Covid 19 is an occupational disease.”2
The INMO strongly welcomed this recognition, viewing it as a critical step in acknowledging both the significant health risks faced by frontline workers and the essential contribution of those in health, social care, and other high-risk occupations during the pandemic.
A Eurostat (2024) survey on the recognition of COVID-19 as an occupational disease found that in the majority of EU Member States, the virus is formally recognised either as an occupational disease or as a workplace accident, therefore entitling affected workers to enhanced protections and compensation. In contrast, Ireland does not formally recognise COVID-19 as either, despite acknowledging that the virus may be associated with workplace exposure.
This places Ireland among a small minority of EU countries that lack clear legal recognition or classification. Sixteen Member States have formally recognised COVID-19 as an occupational disease, while a further eight allow for recognition either as an occupational disease or a workplace accident, depending on national criteria.
The findings of the Eurostat survey are stark, highlighting that Ireland lags behind its European counterparts in formally recognising COVID-19 as an occupational illness or injury. The Government’s reluctance to adopt such a classification appears rooted in a desire to avoid the obligations such a designation would impose on the State and public service employers. This reluctance not only undermines the lived experiences of frontline healthcare workers but also denies them the protections and recognition available to their peers across much of the EU.
Recommendation: In line with the European Commission, the Government must formally classify COVID-19 as an occupational illness or injury.
Environmental Factors: Air Quality and Workplace Safety
As COVID-19 is an airborne pathogen, maintaining high indoor air quality is vital to protect the health and wellbeing of workers.
The INMO consistently rejected the rationale provided by the HSE for its ongoing refusal to apply the precautionary principle and implement air filtration units across all healthcare work locations. This issue was raised repeatedly throughout the pandemic, particularly in settings where poor air quality was frequently reported, such as corridor waiting areas without windows, clinical preparation rooms, wards, and overcrowded emergency and outpatient departments.
CO₂ level monitoring was inadequate throughout and remained so even as the pandemic progressed. During winter, natural ventilation was further compromised due to increased heating, creating conditions that heightened the risk of airborne infection transmission across all areas. (Ref: Letter to Dr Colm Henry, Chief Clinical Officer, Re: Monitoring and Filtration of Air in Health Care Settings, 5 January 2022; PR: INMO repeats calls for curtailment of non-emergency services, Saturday 1 January 2022; Letter to Mr Liam Woods, National Director of Acute Hospitals. Re: Meeting 6 July, 9 July 2021).
Similarly, in its opening statement to the Joint Committee on Health on the Welfare and Safety of Workers in the Public Health Service (INMO, 2022), the INMO again reiterated its concerns for members who worked throughout the pandemic in environments with poor air quality and without effective preventative measures in place. Equally, it was noted that issues that repeatedly emerged in the context of virus transmission amongst staff were inadequate facilities for staff, including changing facilities, break rooms and small offices.
Therefore, the HSE and other healthcare employers must act in the best interest of patients and staff to ensure appropriate environmental conditions, including air quality, in such settings.
A key solution must be to implement air filtration systems in environments where potentially infected air is present and where no adequate ventilation or filtration exists. Given that such systems were introduced in educational settings, it is unreasonable that they were not equally prioritised in healthcare environments where confirmed COVID-19 cases occurred.
While the INMO broadly welcomes the introduction of the HSA’s Code of Practice for Indoor Air Quality, it is equally essential to ensure that employers develop and implement comprehensive air quality policies across all healthcare settings.
Furthermore, a long-term strategy must be established to ensure that Irish hospitals and other healthcare facilities, including residential care and community-based settings, are designed to uphold best practices in IPC and to withstand future outbreaks or pandemics.
Recommedation: The HSE and other healthcare employers must install effective air infiltration systems as part of a long-term strategy to maintain high air quality standards for both patients and staff.
The Experience of Student Nurses and Midwives
The pandemic fundamentally altered the clinical placement experience for student nurses and midwives. They faced increased risks, financial strain due to additional costs and the loss of alternative income sources, and were often required to take on essential work responsibilities owing to COVID related staff absences. Clinical placement suspensions also created uncertainty regarding academic progression. An agreement reached with the Department of Health in March 2020 sought to address some of these workplace-related risks, including the need to provide a safe working environment and to extend protections equivalent to those afforded to employed colleagues facing the same extraordinary risks. Throughout, the INMO consistently emphasised that unpaid students, without a contract of employment, were denied access to basic employment rights.” (Ref: Letter to Mr Stephen Donnelly TD, Minister for Health. Re: Role of Student Nurses/Midwives in Current Climate, 5 February 2021
Unfortunately, there was a clear lack of due care for the health and safety of student nurses and midwives. Information and consultation protocols, which require engagement on such critical matters, were not upheld in interactions with the Department of Health. While some concerns related to wage payments fell under education policy, the pandemic represented an exceptional circumstance where flexibility should have been applied. Health and safety considerations should have taken precedence over long-term policy concerns.
The oversight group failed to propose viable alternatives to meet students’ educational needs and instead endorsed a disorganised and inequitable return to clinical placement. This fragmented class cohorts and disproportionately impacted students whose placements had been disrupted by the pandemic. Ultimately, nursing and midwifery students were uniquely burdened by the educational consequences of these decisions.
Safeguarding the emerging nursing and midwifery workforce is essential—not only for the long-term recovery of the health service post-COVID-19 but also to ensure resilience in the face of future public health emergencies. Protecting these future professionals must be a strategic priority.
Recommendation: The health, safety, and welfare of student nurses and midwives must be embedded as a core priority within workforce planning and pandemic preparedness frameworks. This includes robust protections, structured support systems, and formal mechanisms for consultation on matters impacting their clinical placements and wellbeing.
Long Covid Absences
In March 2020, the Department of Public Expenditure and Reform (DPER) introduced special leave with pay (SLWP) for civil and public servants affected by COVID-19. While the Government initially acknowledged the seriousness of COVID and Long COVID and pledged support for frontline workers, that commitment has since waned. The SLWP scheme was gradually scaled back, most notably impacting healthcare workers who contracted COVID in the workplace after 7 February 2022. Their eligibility for paid leave was capped, even if they remained unfit for work due to debilitating, long-term symptoms.
On 19 July 2022, the HSE introduced a Temporary Scheme of Paid Leave for public health service employees suffering from Long COVID who were no longer eligible for SLWP. Implemented in line with updated DPER guidance, the scheme was introduced without prior consultation with health service unions. Eligibility was restricted to those who had been in receipt of SLWP for at least 84 days prior to 7 February 2022. The scheme underwent multiple short-term extensions, ranging from three to twelve months, creating ongoing financial uncertainty and distress for affected workers.
The INMO along with other health service unions have been seeking the establishment of an occupational illness scheme for healthcare workers who contracted COVID-19 at work and later developed Long COVID, aligned with existing long-term absence schemes in the public health service. The unions are also seeking equitable treatment for workers excluded from support based solely on the date of infection, a criterion that is arbitrary and unjust given the confirmed occupational nature of the illness.
This claim was brought before the Labour Court, which issued its Recommendation on 26 June. The Court held that, as COVID-19 and Long COVID are not currently recognised as occupational illnesses or injuries in this jurisdiction, it does not have the authority to make such a determination. On this basis, it recommended a final extension of the current temporary scheme until 31 December 2025, after which all remaining participants should transition to the standard Public Service Sick Leave Scheme.
Healthcare workers faced the highest risk throughout the pandemic to keep essential services running. Some who contracted COVID in the workplace continue to suffer debilitating symptoms that significantly limit their ability to carry out basic daily activities or spend extended time outside their homes. These workers must be protected, not only those affected during this crisis, but also those who may be exposed in future outbreaks of COVID-19 or other emerging pathogens. No healthcare worker who becomes seriously ill in the course of their duty should have to endure the same stress and uncertainty that Long Covid sufferers have had to face.
Recommendation: The Government must recognise COVID-19 as an occupational illness or injury, as this is essential to removing the barriers identified by the Labour Court that currently prevent the establishment of a permanent Occupational Illness Scheme for healthcare workers with Long COVID. This scheme should be developed in full consultation with health sector unions and aligned with existing public service long term absence frameworks.
Healthcare Environment
Re-emerging Overcrowding
As previously outlined, Ireland’s healthcare system continues to face serious capacity challenges, most notably severe overcrowding in EDs and acute hospitals, an issue the INMO has consistently highlighted.
While the pandemic temporarily eased pressures on EDs and acute services due to reduced activity, overcrowding quickly returned as services resumed.
The INMO and the IAEM, issuing a joint statement in 2020, identified the required actions to ensure appropriate care in EDs and acute health services in the future:
- Emergency Departments and hospital wards must:
- not become reservoirs of healthcare acquired infection for patients
- not become crowded again
- be safe workplaces for all staff
- ED care must be designed and resourced to look after vulnerable patients safely.
As the country faced successive COVID-19 surges, the stark realities of delivering both COVID and non-COVID care in increasingly overcrowded and unsafe environments became clear. Increasingly overcrowded hospitals and poorly ventilated clinical spaces put immense strain on our members and put patient safety and care at risk. Despite calls for appropriate interventions, including an urgent meeting of the ED Taskforce to address the growing concerns of risk of infection, these calls did not see meaningful action. (PR: INMO calls for emergency Taskforce meeting, Friday 18 June 2021). and
The INMO repeatedly raised these concerns, highlighting that the rise in hospital-acquired COVID-19 outbreaks was entirely predictable given the working conditions, stressing the urgent need to mitigate worsening conditions to protect both staff and patients. (Ref: Letter to Dr Tony Holohan, CMO, re: Mask Wearing, 24 March 2022; Letter to Dr Colm Henry, CCO, re: INMO COVID-19 concerns, 5 July 2022).
University Hospital Limerick (UHL), in particular, experienced an alarming rise in overcrowding, with 15.2% of all national trolley figures recorded at UHL alone. The INMO, again, raised this issue repeatedly with senior HSE officials. (Ref: Letter to Mr Liam Woods, National Director of Acute Hospitals, 9 July 2021; Letter to Ms Anne O’Connor, COO, HSE, 5 May 2020 26 January 2022).
In 2022, the decision to remove mandatory mask-wearing further compounded risks. While measures like mask-wearing was one element of IPC guidance, they were vital in containing further spread. The INMO warned that this policy shift, amid rising overcrowding and mounting service pressures, would undermine the safety of both patients and HCWs. (Ref: Letter to Mr Stephen Donnelly TD, Minister for Health, re: NPHET mask-wearing advice, 18 February 2022).
Recommendation: There must be strict adherence to 85% occupancy of acute hospitals and zero tolerance of hospital and emergency department overcrowding.
Lessons Learned and Recommendations
Conclusion
References
1 S.I. 370 of 2016
2 the Commission’s Communication was titled the Strategic Framework on Health and Safety at Work 2020-2027 – Occupational Safety and Health in a Changing World of Work and was published on 28 June 2021 (Document SWD (2021) 149 Final)